History of Surgery Part 6 – Anaesthesia and Analgesia in Ancient Indian Surgery
Anesthesia is a “reversible loss of sensation,” according to Sangyaharana. Surgeons have long understood the benefits of anaesthetic and strived to provide a pain-free operating environment.1 In India, as in other multicultural countries, healing spells and mantras replaced conventional treatment. The main figure in Indian medicine was a priest by the name of Bhisag Atharvan, who had social standing above that of a doctor. The dark, blind, primitive tribes who lived there regularly assaulted the earliest known Aryan settlements in the Punjab. Throughout the war, the doctors routinely treated the Aryan commanders and soldiers. The outcome was that the Aryan warriors’ limbs were stripped of their arrow shafts, their legs were amputated and replaced with iron prostheses, and their damaged eyes were removed.
Sushruta’s approach to anaesthesia, although not as advanced as modern techniques, was innovative. He used herbal anaesthetics such as opium (Ahiphena) and cannabis (Vijaya) to manage pain, employing methods such as inhalation, oral consumption, and topical application. Proper preparation and dosage were crucial, and Sushruta provided detailed guidelines for extracting and administering these herbal remedies. He also employed complementary techniques, such as distraction and positioning, to enhance patient comfort. Despite limitations such as variable efficacy and the short duration of these anaesthetics, Sushruta’s methods laid an early foundation for the pain management practices seen in modern surgery. His foundational Ayurvedic text outlines the use of Madyapanam (intoxicating drinks such as wine) combined with herbal medicines (sedatives), including Cannabis sativa (Bhang), Acorus calamus (Vacha), Nardostachysjatamansi (Jatamansi), Hyoscyamus niger (ParasikaYavani), and others to induce insensibility and pain relief. Sushruta’s pioneering approach to pain management not only enabled over 300 types of surgical operations—including rhinoplasty, cataract extraction, and intestinal repairs—but also introduced the first systematic preoperative, operative, and postoperative protocols emphasizing patient comfort, safety, and consent.
According to the Bhoja-Prabandha (a 17th-century collection of stories), the 11th-century Paramara king Raja Bhoja underwent a successful brain surgery to remove a tumor. Two surgeons from Ujjain reportedly used anesthetic powder (moha-churna) to make him unconscious, opened his skull, removed the growth, and used a revitalizing powder (sanjivani) to wake him. King Bhoja had incurable headaches. All the doctors in the town tried their hands and nothing worked. Having heard about the king’s health problems two Brahmin surgeons from Ujjain came to Dhara and told the king that they can cure him but it involved surgery in the skull. The king told them that he was ready to undergo any difficulty to get out of this torturous headache.
The surgeons brought with them a herb called Sammohini which will put any one in a coma stage like the Chloroform of modern operation theatres. The surgeons know how much of herb to give for certain number of hours. Nowadays the anaesthetists stand by the surgeons to increase the level of chloroform or reduce it. But in those days the surgeons themselves handled this. When the operation was over they administered an antidote herb called Sanjeevini (we have already heard about it in Valmiki Ramayana which cured Lakshmana from Indrajit’s biological warfare). King Bhoja also went through all the procedures, and the surgery was 100 percent successful. He came out of the surgery room as if he had just woken up. This is in Bhoja Prabandham, a Sanskrit book giving his life history.
The modern era of anaesthesia in India began when James Esdaile practiced mesmerism-assisted surgery in Hooghly. However, ether soon took precedence due to its reliability.

James Esdaile (1808–1859)
In 1839, Assistant Surgeon Dr. James Esdaile, in the East India Company’s service, arrived in Hooghly, a town 38 km upriver of Kolkata (Calcutta), to work at Hooghly Hospital. Originally from Scotland—and with a degree in medicine from Edinburgh—Esdaile was advised that a warmer climate would better suit his delicate lungs. In Bengal, Esdaile read about mesmerism, or animal magnetism. The practice, first popularized by Franz Mesmer in the late eighteenth century and only becoming popular in Britain in the nineteenth century, was said to have anesthetic properties and could treat psychoses (“nervous” patients).
Textbook on Mesmerism as an anaesthetic and Curative agent by James Esdaile 1852
As Esdaile described in his book, “Mesmerism in India, and Its Practical Application in Surgery and Medicine,” in April 1845, a local man named Madhab Kaura was sent to him from Hooghly jail for scrotal surgery. Witnessing the patient’s suffering during the procedure, Esdaile allegedly “turned to the native sub-assistant surgeon, an student of the medical college, and asked him if he had ever seen Mesmerism? He said that he had seen it tried at the medical college, but without effect.”
Esdaile admitted that he only knew about the practice from reading, but felt there was nothing to lose by trying it. Although the dulling of pain and loss of senses took longer than he had hoped, it reportedly worked. “I placed [the patient’s] knees between mine,” he reported, “and began to pass my hands slowly over his face, at the distance of one inch, and carried them down to the pit of his stomach. This was continued for half an hour…” Though the pain dulling and sensory loss took longer than expected, it seemed effective. Esdaile even went so far as to “apply” fire to the patient’s knee to test the strength of the trance-like state. The patient remained free of pain.
Esdaile performed seventy-two more operations that year, using mesmerism as an analgesia. A government-appointed committee—composed of colonial Bengal’s most distinguished people, including magistrates and the Inspector General of Hospitals—then allowed him to run an experimental mesmeric hospital, subject to scrutiny from medical officers.
Esdaile’s practice was widely popular with “the natives,” as he termed them, and caused much fanfare. As historian of psychiatry Waltraud Ernst reports, he performed fantastical feats such as excising a tumor “7 feet in circumference and 2 feet at the neck,” seemingly without the patient feeling pain. Historian Alan Gauld writes that Esdaile conducted hundreds of surgeries and reported a 5 percent mortality rate (other techniques had a 50 percent or higher mortality rate).
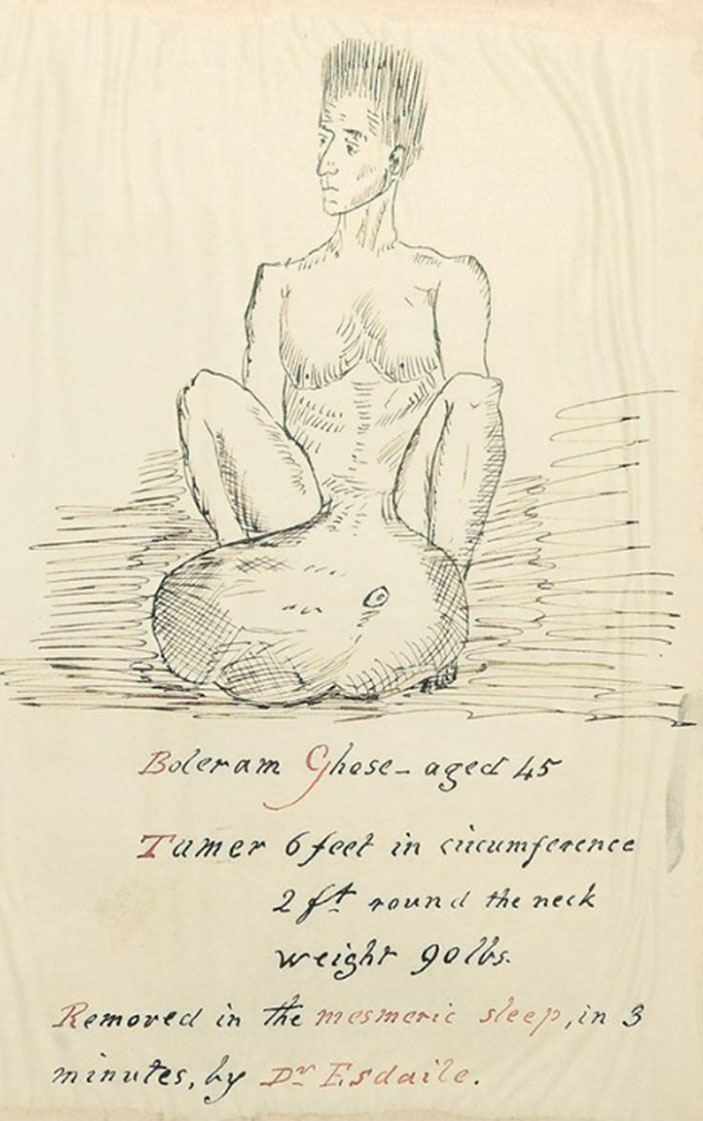
Filarial scrotum Surgery done in 3 minutes by Dr James Esdaile with Mesmerism anaesthesia
Hooghly Hospital came to be called jadoo hospital (the word for “magic” in many Indian languages), less because they believed Esdaile was casting spells and more because of his own use of the phrase belatee munter, “the European Charm,” when explaining mesmerism to Indian assistants.
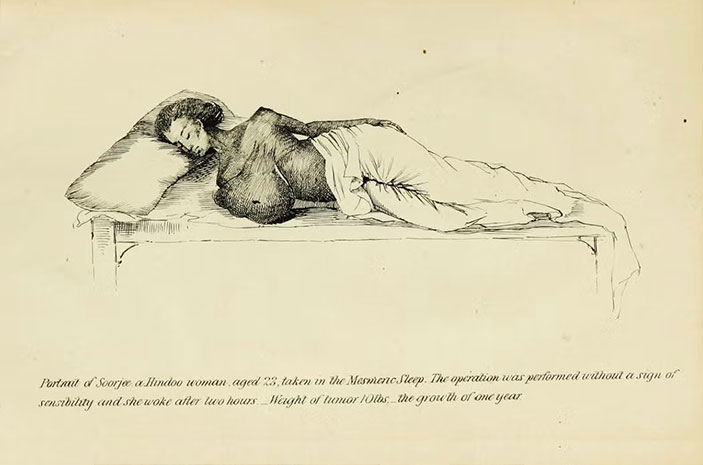
Breast tumour of 10lbs weight removed by James Esdaile by Mesmerism
Despite the initial approval for Esdaile’s experiments by the review committee, mesmerism was widely viewed as a pseudoscience that was nothing but a spectacle for the elite of Europe. At his experimental hospital, Esdaile hired native assistants to perform the mesmerism in his stead (he said the practice tired him excessively). The mesmerizer would take the patients to a dark room and blow over their bodies until they achieved a sleep-like state. Esdaile would come and confirm if the mesmerism was complete. Mesmerism could take days, if not weeks. Once achieved, Esdaile would perform the surgery. The doctors inspecting Esdaile’s work noted that each mesmerizer had their own way of performing the entrancement. It was impossible to standardize . But this wasn’t the only problem. The association of mesmerism with magic was too close. And Esdaile wanted to distance himself from faith healing and present mesmerism as a science.
He did this in part by treating “non-natives,” i.e., Europeans, to legitimize his practice as science. But he also made his practice open to public opinion and reported the results of his experiments in the local newspapers, all to ensure that his work was seen as a science. When Esdaile cured severe epilepsy of the wife of Hooghly’s Deputy Magistrate, Iswar Ghosals, his fame knew no end. Soon, never-ending queues at the hospital became a regular feature with everyone wanting to be part of Dr. Esdaile’s “miracle”.
The government learned about Esdaile’s successes in Hooghly, and decided to give him one year to practice in a controlled environment in Calcutta, where medical observers could watch his operations and write an official report on whether mesmerism worked. The result of the report was mixed; the Governor-General Lord Dalhousie, while generally supportive, decided that it was not worth continuing a Mesmeric Hospital on the government dime.
This is where it gets really interesting. In response to Dalhousie’s decision, the group of locals listed in the second image sent a petition to keep the hospital open – and when that didn’t work, they raised funds through public subscription to create a Mesmeric Hospital for Esdaile! This hospital was located in Creek Row in Central Calcutta, and opened on September 1, 1848. Unfortunately, it did not last long, and Esdaile returned to England in 1851.
The ultimate cause of the demise of Calcutta’s mesmeric hospital was twofold. First, mainstream medicine decided that mesmerism was no more than parlour tricks. And second, the invention of anesthesia made a reliable, much cheaper alternative to mesmerism available – and the East India Company of course went with the cost-saving option.
Most of Esdaile’s patients were Indians, drawn from the general or convict populations. In Mesmerism in India, he described those he treated as coming from a “feeble-minded, ill-nourished race, remarkably deficient in nervous energy.” Eventually, Esdaile’s mesmerism hospital failed due to factors more practical than magical: economics and scientific discovery.
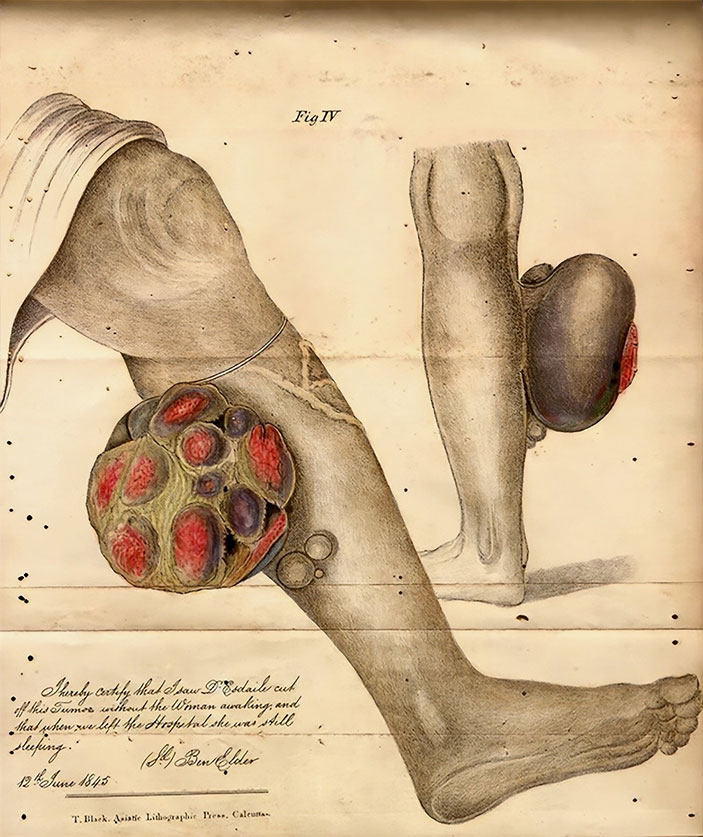
Soft tissue sarcoma surgery by Dr James Esdaile by Mesmerism
Whatever its efficacy, mesmerism was a costly practice. Ernst writes that Assistant Surgeon Dr. Frederic J. Mouat, already a critic of Esdaile, calculated the hospital would incur a significant additional expense of 750 rupees per month with its use, as one mesmerizer was needed for every four patients.
In addition, ether and chloroform were in use by the late 1840s, and they were cheaper, more efficient, and aligned with orthodox Western medical practices. Even Esdaile had to concede, albeit reluctantly, that they were better.
Esdaile was made Presidency Surgeon in 1848, but his mesmeric hospital lost favor. He returned to Scotland in 1851. Though it’s not certain that subtropical Bengal had helped his lungs, Gauld suggests that Esdaile moved once more, south to Sydenham (London), as the Scottish climate “proved too bracing for the weak lungs which had sent him to India in the first place.” He died there in 1859 at the age of fifty-one.
The final conclusion of Mesmerism for surgery, according to Esdaile was “ I beg, to state, for the satisfaction of those who have not yet a practical knowledge of the subject, that I have seen no bad consequences whatever arise from persons being operated on when in the mesmeric trance.
Cases have occurred in which no pain has been felt subsequent to the operation even; the wounds healing in a few days by the first intention; and in the rest, I have seen no indications of any injury being done to the constitution.
On the contrary, it appears to me to have been saved, and that less constitutional disturbance has followed than under ordinary circumstances.
There has not been a death among the cases operated on.”

Hooghly Imambara ( James Esdaile had a hospital in this complex)
Quiz time
Who was the anaesthesiologist for Mahatma Gandhi’s emergent appendicectomy?
Answer – Dr. Date
History of Surgery ASI team
Dr Kaushik Bhattacharya (Head of the team)
Dr Pratap Varute
Dr Patta Radhakrishna
Dr Surajit Bhattacharya
Dr Clement Rajan
Dr K Lakshman
Dr Mahesh Prabhu